Balloon Kyphoplasty Procedure / Vertebroplasty
For Pain Relief
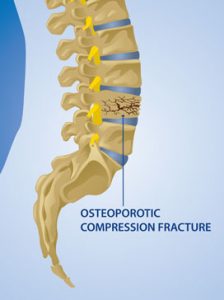
Osteoporosis, which is weakening and thinning of the bone, often has a dramatic impact on the spine, and patients can experience significant compression fractures from osteoporosis. In the past, patients would often have to wear braces for several months.
More recently, kyphoplasty has been developed in which the neurosurgeon is able to expand some of the compression of the bone in the spine and fill the cavity with spinal bone cement. This helps to restore some of the angulation of the spine, restore height, and relieve pain. The success rate of this procedure is very good.
Techniques of Kyphoplasty

1. The normal bones of the spine (thoracic or lumber) have a rectangular appearance, as is seen here. On top of, and below the bone, are the intervertebral disc spaces.
2. When a bone in the spine becomes weak, as happens in the case of aging, it may have an increased risk of fracture. This fracture typically takes on the appearance in which the endplates on the top and bottom of the vertebral body come closer together. This is typically the appearance of an osteoporotic compression fracture. A compression fracture may also occur when there is a tumor within the substance of the vertebral body, and this is known as a pathologic fracture.


3. During the kyphoplasty procedure, an opening is made, through the skin, into the pedicle, and subsequently into the vertebral body of the spine. The hole is large enough to pass a small balloon.
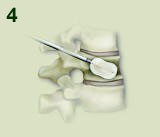
4. Once the balloon is inserted, it is inflated, to expand the vertebral body, and “reduce” the spinal osteoporotic compression fracture.

5. Once the cavity has been created in the osteoporotic spinal bone, the balloon is removed, leaving a hollow space.
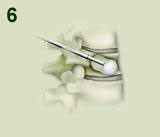
6. The cavity of the spinal osteoporotic compression fracture is then filled, in a low-pressure manner, with cement.

7. When the cement hardens inside the spinal osteoporotic compression fracture, an internal cast is created. This internal cast will provide additional substance and support to the osteoporotic compression fracture, resulting in decreased pain in most cases. Once the cement is hard, the patient can get up and assume most of his/her activities. Of course, the adjacent bones are still weak, and care must be taken to avoid injury to those levels.
Patients may choose to have kyphoplasty performed if they are experiencing pain in the spine associated with an osteoporotic compression fracture of the spine.
Before the operation begins, the anesthesiologist will put the patient to sleep. The patient is then carefully positioned on their abdomen in the operating room and the area of the back where the procedure is to occur is prepared in a sterile manner.
The neurosurgeon uses live x-ray (fluoroscopy) extensively during the procedure. Two different x-ray machines (C arms) are used at the same time to allow the neurosurgeon immediate visualization of the procedure from the AP view (front to back of the patient) and the lateral view.
The neurosurgeon first places a needle and then a small drill into the vertebral body through the pedicle of the vertebral body. The neurosurgeon then passes a balloon into the compressed vertebral body in order to expand the body and correct some of the angulation and loss of height.
After doing this on both sides, the neurosurgeon then injects cement under low pressure into the vertebral body. This cement hardens within minutes, and then the physician removes the needles. Finally, the skin is closed with glue.
A vertebroplasty is performed in a similar manner, without the use of balloons to expand the crushed vertebral body.
Patients are generally discharged home an hour or two after the procedure is performed; however, a friend or family member must drive them.
The puncture sites on the back should be kept clean and dry for several days; otherwise, they can resume their normal activity. They should remember, however, that they still have osteoporosis and, with excessive lifting, other bones in the spine may be at risk of fracture.
The risks of kyphoplasty and vertebroplasty are very low. Potential risks include bleeding, infection, nerve injury, spinal cord injury, leakage of cement around the spinal nerves or spinal cord, embolization of cement into the veins and ultimately into the lungs, coma and death.